 |

Neurological
Basis of Behavior (PSY -
610)
VU
Lesson32
Basic
Neurochemistry
Objectives:
To
familiarize the students with
the
Various
NT and their role in the modulation of
behaviors
Classification
of Neurotransmitters. Monoamines:
Catechoalimnes
and
Indolemaine,
acetylcholine,
amino acid, and Peptide
Neurotransmitters
role in modulation of behaviors and
Aberration
Drugs
and Behavior:
Classification
of Psychopharmacological substances
Behavioral
correlates, Treatment:
Mechanism
of synaptic transmission
Major
Neurotransmitters:
Catecholamines:
Dopamine
Dopamine
(DA) a major catecholaminergic
neurtotranmitter was discovered by
Udenfriend in 1964.
This
is the first step in the synthesis
chain of the Adrenergic ( also
known as Epinephrine) and
Noradrenergic
(also known as Norepinephrine) NT
systems, however, this was
the last to be given the
status
of an NT, because DA was thought to be
only an intermediatary step in the
synthesis of
Norepinephrine.
Dopamine has been found to
have a major influence on behavior,
especially motor
behavior
and schizophrenia. These chemical are
also found in the body, in the adrenal
glands and used
in
the sympathetic action in emotional
states; however, whatever is produced in
the body cannot cross
the
blood-brain barrier to get into the
brain. The brain is very
well protected (as you have
seen in the last
module).
In order to keep the environment
sterilized, the brain manufactures
all the chemicals it
needs
from
the precursors (the first compound in the
chain, which can then be
acted upon by enzymes).
The
precursors
are taken in from the blood
circulation.
The
Synthesis chain of DA, NE and E begins
with tyrosine (we will
discuss this in detail
later.
DA
has two types of receptors in the
brain the D1 and D2
D1.are
linked to the stimulation of the
adenylate cyclase. These are
present in thew Corpus Straitum
and
the
Butrypheneones (a class of drugs known as
neuroleptics, anitpsychotics) are
weak antagonist for
these
receptors.
D2.
These
are linked to the inhibition of
adenylate cyclase. These are
present in the pituitary and
the
Corpus
striatum. The Butryphenones
are potent antagonists for
these receptors
DA
Pathways: There are three
major pathways of this
system
1.
The
Nigrostriatal DA system. This is
largest and longest bundle of fibers of
neurons containing
DA.
This
is a major tract which has
80% of brain's Dopamine It
originates in the Zona
Compacta of
Substantia
Nigra and sends projections to the Corpus
Striatum. The degeneration of
this systems leads to
Parkinson's
disease (a major motor
disorder in which voluntary
movements become
increasingly
difficult
and there are only some
stereotypic movements seen).
This is also involved in
schizophrenia.
Reduced
levels of DA in this system
lead to Parkinson's disease
and increased levels lead
to
schizophrenic
symtoms.
2.
Mesolimbic: This is a
medially located diffuse (wide
spread out projections)
systems. This system
sends
out nerve fibers which go
out to the forebrain areas
such as frontal cortical
area, the cingulated
cortex,
the amygdale and the septum. As the names
implies this is involved
with the limbic
system
116
Neurological
Basis of Behavior (PSY -
610)
VU
(emotional
system). The anti psychotics drugs
act here to reduce the
apathy and lack of
affect
(emotional
content) which is characteristic of
schizophrenia.
3.
Tuberoinfundibular: This is
also known as the hypothlamic
hypophyseal connection. It
originates
from
arcuate and periventricular regions of
hypothalamus, and there are very short
fibres which end up
in
the intermediate lobe of the pituitary.
This appears to play a role
in the hormonal controls
and
modulations.
Dopamine
is also found in other areas
in the brain
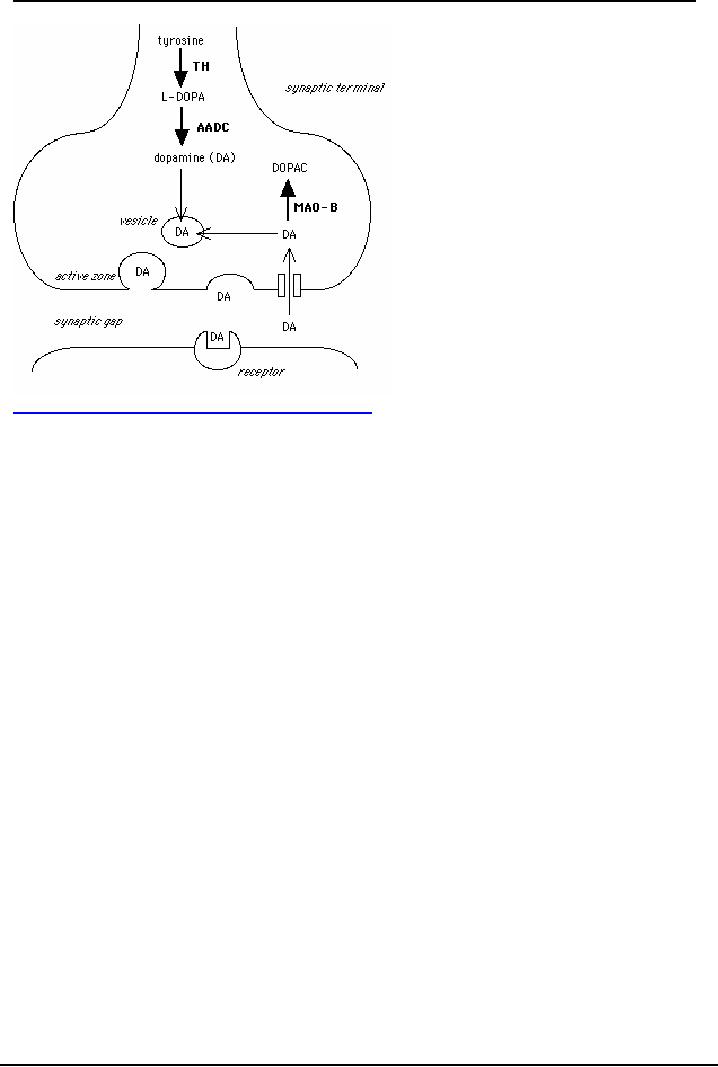
Synthesis
Pathway. As a
rule it must be remembered
that the brain manufactures
its own
neurochemicals
including Dopamine from the precursor
taken in from the blood
supply (circulatory
system).
1.
Phylalanine which is
taken in from food and is
immediately hydroxylated (add a
hydroxyl molecule)
by
the enzyme phylalanine hydroxylase to
convert to Tyrosine
2.
Tyrosine: tyrosine is
then immediately hydroxylated
by
tyrosine
hydroxylase. This is known as
the
rate
limiting step (and is
sensitive to pharamoclogical
manipulations), we can control the amount
of DA
(as
well as NE, and E) manufactured in the
systems. This hydroxylation
leads to the formation of
DOPA
3.
Dopa: This is
similar to a drug known as
L-Dopa, effective in the treatment of
Parkinson's. Dopa is
then
decarboxylated (removal of the carboxyl
molecule) by the enzyme dopa decarboxylase, to
form
Dopamine
4.
Metabolic degradation:
a)
Dopamine
is then metabolized by Monoamine Oxidase
(MAO)
which
converts monoamines to
aldehydes
to make them inactive. Monoamine oxidase is
not specific for dopamine,
but acts on all
mono
amines
NE, E, and serotonin. This is
found in the presynaptic
region.
b)
COMT- catechol O
methyl transferase, acts to transfer the
methyl from the catechol
molecule to
deactivate
it. This is found in the
synaptic cleft as well as the
presynaptic areas
117
Neurological
Basis of Behavior (PSY -
610)
VU
http://tcw2.ppsw.rug.nl/~vdbosch/pd.html#Heading18
Pharmacological
interventions: Step where
DA synthesis pathway can be
blocked or altered
It
is clear that pharmaceutical substances/ drugs
act in the central nervous systems
through the
neurchemical
systems.
Agonists:
are
drugs that copy / mimic the
action of the neurotransmitter or have
similar effect as the NT
or
have an excitatory effect on the NT
systems.
Antagonists:
are drugs that block,
inhibits or in any way
opposes the action of the NT.
Drugs:
or exogenously administered substances
can affect the NT pathway at
various levels
a)
They
can act directly on neurons
containing the NT
b)
They
can act on various points of
the synthesis pathway the pre-post receptor
site
c)
They
can act on the inactivating
enzymes in the cleft or within the
presynaptic area.
Steps
where drugs can interact in
the synthesis
pathway
Step
1.
This is first step in the precursor
transportation pathway within the
neuron. Phenlalanine has
to
be
hydroxylated to form tyrosine
which would then be
available for the synthesis
into DA. However,
this
conversion can be blocked as in the
case of the genetic disorder
PKU (phenylketunuria) where
Phenylalanine
is build up and transforms into toxics
which damage the brain cell.
The PKU buildup
blocks
the transport of both tyrosine and
tryptophan in the brain. Therefore no
tyrosine, no DA!
Step
2: This
is where the enzymatic synthesis of Dopamine begins.
Tyrosine is the first amino
acid in
the
chain of metabolism of catecholamines
and is the most susceptible to blockade.
The hydroxylation
action
can be blocked by A-Methyl
Para Tyrosine (AMPT) which
methylates the tyrosine (instead of
hydroxylation).
This reduces the level of
Tyrosine available, which
then leads to reduced
Dopamine,
Norepinephrine
and, Epinephrine. AMPT is effective in
reducing catecholamine levels in the
brain.
Step
3: Conversion
of DOPA into dopamine by dopa
decarboxylase can be blocked by a false
enzyme
A-methyl
dopa. This enzyme competes
for DOPA and uses it so that
it cannot be converted in the
correct
form in order to become
dopamine
118

Neurological
Basis of Behavior (PSY -
610)
VU
Step
4: Storage
vesicles: The storage vesicles
are packed with Dopamine. Reserpine, a
drug
manufactured
from Rauwolfia Alkaloids is
classified as a major and
long lasting tranquilizer.
Reserpine
ruptures
all vesicles irreversibly and the
contents get spilled out
into the presynaptic area where
they get
deactivated
if they do not get out into
the synaptic cleft. These
vesicles cannot be repaired till
new
vesicles
are manufactured; therefore no DA
molecules can store. Another
drug, Tetrabenazine
also
opens
up the vesicles and blocks reuptake of DA
into the vesicles. However, this is
not irreversible as
the
vesicles are not ruptured
only opened up.
Step
5.
This is where the release of the Nt for
the presynaptic ending, and the
reuptake back form the
synaptic
cleft can be blocked. The
drug Amphetamine (a stimulant)
releases and blocks the reuptake
of
DA
for a prolonged agonistic
action. Similarly, Cocaine (another
stimulant, and street drug)
and
Tricyclic
group of antidepressant also
block reuptake of DA,
NE
Step
6. Action within the
neuron, axonal
ending and the synaptic cleft.
The deactivation process
can
be
blocked by drugs which block
action of MAO. The drug
Pargyline, and MAOI, can
increase amount
of
DA available by blocking the deaminating
process (blocking the
blocker!).
Step
7. The
post receptor site-can also be blocked or
stimulated. Apomorphine is a DA
receptor
stimulant
at pre and post receptor sites
and thereby increases the
levels of DA available for
action.
Haloperidol
which is a potent antipsychotic
drug is a DA blocking agent.
Therefore
drugs can be used to modify the
action of the neurochemcicals at the various
sites of synthesis
pathways.
DA
and Behaviors
The
behaviors that are affected
or modulated by the DA systems would be
discussed in details
Dopamine
and Motor
Activities:
SN
and Corpus Striatum. The
Dopaminergic Nigrostrial system is
atypical in the CNS format
that SN
fibers
do not cross over to the
contralteal hemispheres i.e.
they remain on the same side
of the brain.
This
system innervates the extrapyramidal
structures (the basal
ganglia) which controls
motor behavior
at
the sub cortical
level.
A)
Damage
to SN leads to Parkinson's disease.
This was first discovered by
pathologists who
reported
that
the SN of Parkinson's patients was pale
as compared to normal brains. The
dopaminergic neurons
in
Substantia Nigra have dark pigmentation;
therefore the pale SN indicates damage to
the DA neurons.
Thus,
reduced levels of DA in SN leads to
Parkinson's symptoms.
Logically
it can be assumed that if we
inject dopamine in these patients we
should see a reduction
in
Parkinson's
symptoms. This is exactly
what happens if we increase
levels of Dopamine by
injecting
Dopa
(or L-Dopa) in SN.
B)
Evidence
that rats injected with
6-OHDA
a
toxic agent which selectively
damages only the DA
pathways
and neurons by retrograde transmission,
exhibit the same symptoms as in
Parkinson's
(rigidity,
tremor, etc). This also indicates
that DA is involved in Parkinson' as
well as motor
behavior
C)
If
DA levels are increased in animals or
humans by injections of L-Dopa, it
leads to stereotypic
(repetitive)
motor behavior. The
stereotypic behavior is a symptom of
higher than normal levels of
DA
in
the brain. In rats we see
repeated running back and forth, or
grooming their faces with
their paws or
any
other motor activity.
Stereotypic behavior is also
seen in human Parkinson's patients who
are
treated
with high doses of L-Dopa.
Furthermore, apomorphine and amphetamine
(both strong agonists
of
DA) at high enough doses
lead to stereotypic
behaviors.
119

Neurological
Basis of Behavior (PSY -
610)
VU
D)
Injections
of Haloperidol& Chloropromazine (anti
psychotic drugs which block
DA activity) block
the
stereotypy induced by the amphetamine
injections. This means the
following:
Increase
DA by amphetamine-> Stereotypy,
Block
DA.by Haloperidol-> Reduce
Amphetamine induced
stereotypy
E)
Unilateral
lesions of 6-OHDA lesions lead to a
symmetry in body postures
that is the body
becomes
lopsided.
The body turns from the side
with high DA to the side
with low DA. This
lopsided body
posture
is exaggerated by amphetamine and apomorphine
(Ungerstedt et al, Najam
1980). So if we
lesion
the right side, the body turns from
left to right (right side
has lost its DA) On the
other hand,
unilateral
electrical stimulation in the intact
brain also lead to same
kind of body asymmetry. If
we
stimulate
the right side, then the posture would be
lopsided from right to left.
The body Postural
asymmetry
is from side with more DA to the
side with lesser DA
F)
Bilateral
Lesions with 6-OHDA lead to a compelte
reduction of DA in the brain. Animals
with
bilateral
lesions do not eat, (aphagia)
drink (adipsia), and cannot survive.
They recover feeding only
is
forcefed.
Dopamine
and Depression
·
It
is very well researched that Antidepressants such as Monoamine oxidase
inhibitors (MAOI)
and
the Tricyclics both increase the levels of DA
·
Alpha
methyl para tyrosine (AMPT) if injected reduces both the NA, DA levels in the
brain. If
we
then inject MOAI, there is reduced effectiveness of the anti depressives effect
of MAOI.
This
indicates that some levels of DA is needed in the brain (However, evidence
indicates that
these
have greater interaction with NA than DA (Desipramine an antidepressant has no
effect on
DA
neurons, and Tricyclics also greater interaction with NA).
Dopamine
and hyperactivity
Hyperactivity
is due to increased levels of dopamine in the brain. This is also seen with
injections of
Amphetamine
and apomorphine.
The
market drug "speed"
is
actually amphetamine, which users
take to feel tireless and
increased
energy
and euphoria (I can conquer the
world feeling!)
Dopamine
and Schizophrenia
There
is strong evidence that DA is involved in Schizophrenia.
a)
Drugs
which are effective in treatment of schizophrenic symptoms are strong DA
blockers. The more
effective
the drug is as a DA blocker, the greater would be its anti psychotic
potency/efficacy in
treating
the symptoms.
b)
The
greater the efficacy of treatment (reducing DA) the greater the side effect of
extrapyramidal
symptoms
(Parkinson's like tremor, rigidity). The extrapyramidal symptoms such as body
tremors
appear
because DA is decreased postsynaptically. The DA synapses are blocked by
these
antipsychotic
drugs such as Phenothiazines (largectil and haloperidol:
haldol)
c)
The
patients of Parkinsons when treated with L-Dopa start exhibiting symptoms of
schizophrenia- as
a
side effect of the treatment
e)
Chronic
users of amphetamine end up with symptoms
of paranoid schizophrenia
120

Neurological
Basis of Behavior (PSY -
610)
VU
Therefore
DA is important in a wide range of behaviors, from motor activity to
schizophrenia
References:
1.
Kalat J.W (1998) Biological
Psychology Brooks/ Cole
Publishing
2.
Carlson N.R. (2005) Foundations of
Physiological Psychology Allyn and Bacon,
Boston
3.
Pinel, John P.J. (2003)
Biopsychology (5th edition) Allyn and Bacon
Singapore
4
Bloom F, Nelson and Lazerson (2001),
Behavioral Neuroscience: Brain, Mind and
Behaviors (3rd
edition)
Worth Publishers New
York
5.
Bridgeman, B (1988) The
Biology of Behaviour and Mind. John
Wiley and Sons New
York
6.
Brown,T.S. and Wallace.(1980) P.M
Physiological Psychology
Academic
Press New York
7.
Seigel, G.J. (Ed. in chief)
Agranoff, B.W, Albers W.R.
and Molinoff, P.B. (Eds) (1989)
Basic
Neurochemistry:
Molecular, Cellular and Medical
Aspects
8.
Cooper,J.R, F.E Bloom,and
R.H Roth (1996) Biochemcial
basis of neuropharmacology 7th
Edition,
OUP
9.
Pharmacology, Biochemistry and
behavior
(Additional
references for the module: Iversen and Iversen, Gazzaniga, Bloom, and
handouts)
Note:
References
2, 3, 4, 7 more closely followed in
addition to the references cited in
text.
121
Table of Contents:
- INTRODUCTION:Descriptive, Experimental and/ or Natural Studies
- BRIEF HISTORICAL REVIEW:Roots of Behavioural Neurosciences
- SUB-SPECIALIZATIONS WITHIN THE BEHAVIORAL NEUROSCIENCES
- RESEARCH IN BEHAVIOURAL NEUROSCIENCES:Animal Subjects, Experimental Method
- EVOLUTIONARY AND GENETIC BASIS OF BEHAVIOUR:Species specific
- EVOLUTIONARY AND GENETIC BASIS OF BEHAVIOUR:Decent With Modification
- EVOLUTIONARY AND GENETIC BASIS OF BEHAVIOUR:Stereoscopic vision
- GENES AND EXPERIENCE:Fixed Pattern, Proteins, Genotype, Phenotypic
- GENES AND EXPERIENCE:Mendelian Genetics, DNA, Sex Influenced Traits
- GENES AND EXPERIENCE:Genetic Basis of behavior, In breeding
- GENES AND EXPERIENCE:Hybrid vigor, Chromosomal Abnormalities
- GENES AND EXPERIENCE:Behavioral Characteristics, Alcoholism
- RESEARCH METHODS AND TECHNIQUES OF ASSESSMENT OF BRAIN FUNCTION
- RESEARCH METHODS AND TECHNIQUES OF ASSESSMENT OF BRAIN FUNCTION:Activating brain
- RESEARCH METHODS AND TECHNIQUES OF ASSESSMENT OF BRAIN FUNCTION:Macro electrodes
- RESEARCH METHODS AND TECHNIQUES OF ASSESSMENT OF BRAIN FUNCTION:Water Mazes.
- DEVELOPMENT OF THE NERVOUS SYSTEM:Operation Head Start
- DEVELOPMENT OF THE NERVOUS SYSTEM:Teratology studies, Aristotle
- DEVELOPMENT OF THE NERVOUS SYSTEM:Stages of development, Neurulation
- DEVELOPMENT OF THE NERVOUS SYSTEM:Cell competition, Synaptic Rearrangement
- DEVELOPMENT OF THE NERVOUS SYSTEM:The issues still remain
- DEVELOPMENT OF THE NERVOUS SYSTEM:Post natal
- DEVELOPMENT OF THE NERVOUS SYSTEM:Oxygen level
- Basic Neuroanatomy:Brain and spinal cord, Glial cells, Oligodendrocytes
- Basic Neuroanatomy:Neuron Structure, Cell Soma, Cytoplasm, Nucleolus
- Basic Neuroanatomy:Control of molecules, Electrical charges, Proximal-distal
- Basic Neuroanatomy:Telencephalon, Mesencephalon. Myelencephalon
- Basic Neuroanatomy:Tegmentum, Substantia Nigra, MID BRAIN areas
- Basic Neuroanatomy:Diencephalon, Hypothalmus, Telencephalon, Frontal Lobe
- Basic Neurochemistry:Neurochemicals, Neuromodulator, Synaptic cleft
- Basic Neurochemistry:Changes in ionic gates, The direct method, Methods of Locating NT
- Basic Neurochemistry:Major Neurotransmitters, Mesolimbic, Metabolic degradation
- Basic Neurochemistry:Norepinephrine/ Noradrenaline, NA synthesis, Noadrenergic Pathways
- Basic Neurochemistry:NA and Feeding, NE and self stimulation: ICS
- Basic Neurochemistry:5HT and Behaviors, Serotonin and sleep, Other behaviours
- Basic Neurochemistry:ACH and Behaviors, Arousal, Drinking, Sham rage and attack
- Brain and Motivational States:Homeostasis, Temperature Regulation, Ectotherms
- Brain and Motivational States:Biological Rhythms, Circadian rhythms, Hunger/Feeding
- Brain and Motivational States:Gastric factors, Lipostatic theory, Neural Control of feeding
- Brain and Motivational States:Resting metabolic state, Individual differences
- Brain and Motivational States:Sleep and Dreams, Characteristics of sleep
- Higher Order Brain functions:Brain correlates, Language, Speech Comprehension
- Higher Order Brain functions:Aphasia and Dyslexia, Aphasias related to speech
- Higher Order Brain Functions:Principle of Mass Action, Long-term memory
- Higher Order Brain Functions:Brain correlates, Handedness, Frontal lobe