 |
MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS |
| << MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS |
| PSYCHOLOGICAL PROBLEMS OF CHILDHOOD:Kinds of Internalizing Disorders >> |
Abnormal
Psychology PSY404
VU
Lesson
43
MENTAL
RETARDATION AND DEVELOPMENTAL
DISORDERS
Developmental
psychopathology is the study of how
disorders arise and change
with time. These
changes
usually follow a pattern, with
child mastering one skill
before acquiring the next, it implies that
any
disruption in the acquisition of early
skills by the very nature of the developmental
process also
disrupt
the development of later skills. Developmental
Psychopathology approach is absolutely
essential
to
disorders of children, because children
change rapidly during the
first 20 years of life.
Psychologists
become
concerned only when a child's behavior
deviates substantially from developmental
norms,
behavior
that is typical for children of a given
age.
1-
Attention Deficit Hyperactivity
Disorder
·
The
primary characteristics of people with
attention deficit hyperactivity disorder
are the pattern
inattention
(such as not paying attention to
school-or work related tasks) or
hyperactivity-
impulsivity,
or both.
·
These
deficits can significantly disrupt
academic efforts and social
relationships.
2-
Learning Disorders
DSM-IV-TR
groups the learning disorders as
·
reading
disorder
·
Mathematics
disorder
·
Disorder
of written expression
All
are defined by performance
that fall far short of
expectations based on intelligence and
school
preparation.
3-
Verbal or communication
disorders
Verbal
or communication disorders seem closely
related to learning disorders.
·
They include
stuttering, stammering, disturbance in
speech fluency, expression,
language disorder, a
very
limited speech in all
situations.
·
Selective
mutism.
4-
Pervasive Developmental
Disorder
·
People
with pervasive developmental disorder
experience trouble progressing in
language,
socialization
and cognition. The use of
word pervasive means that
these are not relatively
minor
problems
(like learning disabilities) but
conditions that significantly affect how
individuals live.
Kinds
of Pervasive Developmental
Disorder
(i)
Autistic Disorder
(ii)
Attention Deficit Hyperactivity
Disorder (ADHD)
(iii)
Oppositional Deficit Disorder
(ODD)
(iv)
Conduct Disorder
(v)
Asperger's Disorder
(vi)
Childhood Disintegrative Disorder
(vii)
Rett's Disorder
·
Mental
retardation and Pervasive Developmental
Disorders (PDD) involve
serious disruptions in
development.
·
Both
disorders are either present at
birth or begin early in
life.
·
Both
affect many areas of intellectual,
social, and life
functioning.
·
Autism
is the most familiar PDD,
and, in fact, professionals
often use the term autistic
spectrum
disorders
as a
synonym for PDD.
213
Abnormal
Psychology PSY404
VU
·
PDD
are distinguished by dramatic, severe,
and unusual symptoms.
·
Socially,
the child not only lives in
a world of his own but
also in a world
apart.
·
Many
children with PDD also
cannot communicate.
·
In
addition, children with PDD
are preoccupied with unusual
repetitive behavior, like
needing to
preserve
rigid routines or rocking back
and forth endlessly.
·
All
people with mental retardation have
impaired intellectual abilities, but they vary widely
in
academic
ability, social functioning,
and life skills.
·
Some
people with profound retardation require
total care and live
their entire lives in
institutions.
·
However,
most people with mental retardation
learn the self-care and vocational
skills that allow
them
to live in the community.
·
All
people with mental retardation have
impaired intellectual abilities, but they vary widely
in
academic
ability, social functioning,
and life skills.
·
Some
people with profound retardation require
total care and live
their entire lives in
institutions.
·
However,
most people with mental retardation
learn the self-care and vocational
skills that allow
them
to live in the community.
·
Pervasive
developmental disorders (PDDs) begin early in
life and involve severe
impairments in a
number
of areas of functioning.
·
People
with PDD exhibit profound
disturbances in relationships, engage in
unusual behaviors,
and
typically
have substantial communication
difficulties.
1-
Autistic Disorder
(Autism)
·
Autistic
disorder (autism) is characterized by
profound indifference to social
relationships, odd,
stereotypical
behaviors, and severely impaired or
nonexistent communication skills.
·
Early
onset is a defining feature of
autism.
·
Because
babies with autism look
normal, the condition may not be
accurately diagnosed for a
few
years,
as infants and toddlers fail to reach
developmental milestones and social
achievement.
·
Communication
problems range from few
difficulties disorder to profound
impairments in many
cases
of autism.
·
According
to field studies conducted
for DSM-IV, 54 percent of
patients with autism remain
mute,
as
do 35 percent of patients with
other PDD.
·
Echolalia is
a common problem.
·
Those
with autism or other PDD
frequently repeat phrases
that are spoken to them, or
sometimes
repeatedly
echo a phrase they heard at an
earlier time.
·
Another
common language problem is
pronoun reversal, which
involves confusing the pronoun
"you"
with the pronoun "I."
·
The
inability to relate to others is another
central feature of autistic
disorder.
·
One
view is that people with
autism lack a theory of
mind--that is, they fail to
appreciate that other
people
have a point of reference
that differs from their
own.
·
Another
defining symptom of autism is
restricted, repetitive, and
stereotyped patterns of
behavior,
interests,
and activities.
·
These
odd preoccupations and rituals
create social
complications.
·
Rituals
such as flapping a string or spinning a
top seem to serve no other
function than
providing
sensory
feedback or self-stimulation.
·
Self-injurious
behavior is one
of the most bizarre and
dangerous difficulties that
can accompany PDD.
Frequency
of Autism and PDD
·
Upper
level estimates now suggest
that as many as 60 in 10,000
children suffer from
autism.
·
Three to
four times as many boys as
girls suffer from autism,
suggesting a gender-linked
etiology.
·
Autism
also is much more common
among siblings of a child
with autism, suggesting
possible
genetic
causes.
214
Abnormal
Psychology PSY404
VU
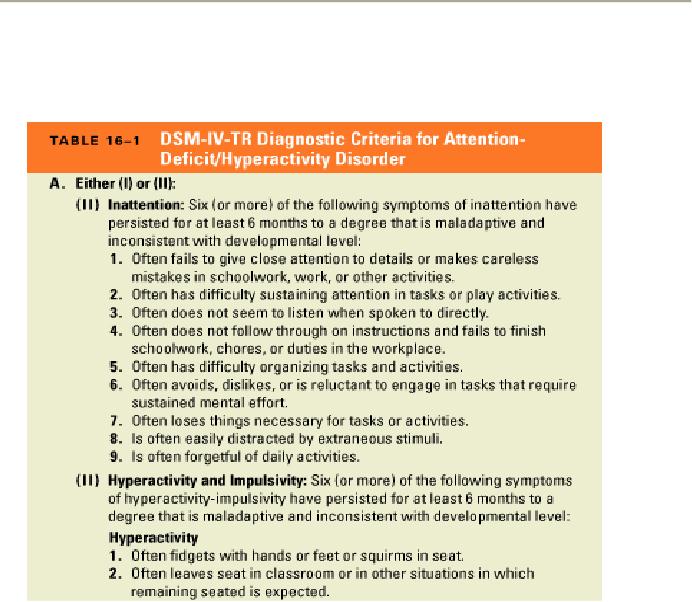
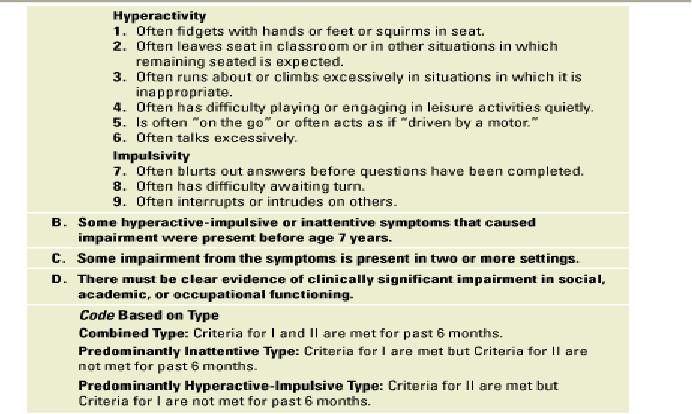
2-
Attention-deficit/hyperactivity disorder
(ADHD)
·
Attention-deficit/hyperactivity
disorder (ADHD) is characterized by
hyperactivity, attention
deficit,
and
impulsivity.
·
The
symptoms of hyperactivity and
attention deficit each have
been viewed as being the core
characteristics
of ADHD.
215
Abnormal
Psychology PSY404
VU
3-Oppositional
Defiant Disorder
(ODD)
·
Oppositional
defiant disorder (ODD) is defined by a
pattern of negative, hostile, and
defiant
behavior.
·
The
rule violations in ODD typically involve
minor transgressions, such as refusing to
obey adult
requests,
arguing, and acting
angry.
·
A pattern of
negativistic, hostile, and defiant
behavior lasting at least 6
months, during which
four
(or
more) of the following are
present:
o
Often
loses temper.
o
Often
argues with adults.
o
Often
actively defies or refuses to comply with
adults' requests or
rules.
o
Often
deliberately annoys people.
o
Often
blames others for his/her
mistakes or misbehavior.
o
Is
often touchy or easily
annoyed by others.
o
Is
often angry and
resentful.
o
Is
often spiteful and
vindictive.
·
The
disturbance in behavior causes clinically
significant impairment in social, academic,
or
occupational
functioning.
·
Note:
Consider
a criterion only if the behavior
occurs more frequently than
is typically observed in
individuals
of comparable age and developmental
level.
·
Professionals
have long debated whether ADHD
and ODD are the same or
separate disorders.
·
The
current consensus is that the two
disorders are separate but
frequently comorbid.
·
Not
only ADHD and ODD are highly
comorbid, but about 25
percent of children with
each
problem
also have a learning disorder.
4-Conduct
Disorder (CD)
·
Conduct
disorder (CD) is defined primarily by a
persistent and repetitive pattern of
serious rule
violations,
most of which are illegal as
well as antisocial--for example,
assault or robbery.
·
DSM-IV-TR
distinguishes the age of onset in
defining conduct disorders--a distinction
between
adolescent-limited
versus life-course patterns of
antisocial behavior.
216

Abnormal
Psychology PSY404
VU
·
Most
of the symptoms of conduct disorder involve
index offenses--crimes against people
or
property
that are illegal at any
age.
·
A
few diagnostic criteria are comparable to
status offenses--acts that are illegal
only because of the
youth's
status as a minor.
·
However,
juvenile delinquency is a legal
classification,
not a mental health
term.
·
Anywhere
from 5 to 15 percent of youth in the
United States may have ODD
and/or CD.
·
After
the first few years of life,
from two to ten times as
many boys as girls have an
externalizing
disorder.
217
Abnormal
Psychology PSY404
VU
·
Except
for the normative increase
during adolescence, the prevalence of
externalizing behavior
generally
declines with age, although
it declines at much earlier
ages for girls than
for boys.
·
Externalizing
disorders are associated
with various indicators of family
adversity, a fact highlighted
by
British psychiatrist Michael
Rutter.
·
Rutter's
Family Adversity Index includes
six family predictors of behavior
problems among
children:
low
income,
overcrowding
in the home,
maternal
depression,
paternal
antisocial behavior,
conflict
between the parents,
and
removal
of the child from the
home.
5-
Asperger's Disorder
The
new diagnosis for Asperger's
disorder refers to people who show the
symptoms of autism but
do
not
have major problems in communication and
generally function higher in other
areas as well.
6-
Childhood Disintegrative
Disorder
Childhood
disintegrative disorder refers to a poorly understood
and somewhat controversial
condition
characterized
by severe problems in social
interaction and communication, in
addition to stereotyped
behavior.
7-
Rett's Disorder
Rett's
disorder is a clearly distinct condition
characterized by at least 5 months of normal
development
followed
by
o
a
deceleration in head
growth,
o
loss
of purposeful hand movements,
o
loss
of social engagement,
o
poor
coordination, and
o
a
marked delay in
language.
Treatment
of PDD (continued)
1-
A huge
variety of medications have been
used to treat autism, including
antipsychotics,
antidepressants,
amphetamines, psychedelics, and
megavitamins.
Unfortunately,
none of these medications is an effective treatment
for autism, and few show
much
promise.
2-
Intensive
behavior modification using operant
conditioning techniques called
Applied
Behavior Analysis
(ABA)
is the
most promising approach to treating
autism.
ABA
therapists focus on treating the specific
symptoms of autism, including
communication deficits,
lack
of self-care skills, and self-stimulatory
or self-destructive behavior.
3-
Behavior
therapists have been fairly
successful in teaching self-care
skills and less successful
in
teaching
social responsiveness.
4-
One of the
most actively researched residential
programs is Achievement
Place, a
group home that
operates
according to highly structured
behavior therapy principles.
Achievement
Place homes, like many
similar residential programs,
are very effective in improving
aggression
and noncompliance while the adolescent is
living in the treatment setting.
218
Table of Contents:
- ABNORMAL PSYCHOLOGY:PSYCHOSIS, Team approach in psychology
- WHAT IS ABNORMAL BEHAVIOR:Dysfunction, Distress, Danger
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Supernatural Model, Biological Model
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Free association, Dream analysis
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Humanistic Model, Classical Conditioning
- RESEARCH METHODS:To Read Research, To Evaluate Research, To increase marketability
- RESEARCH DESIGNS:Types of Variables, Confounding variables or extraneous
- EXPERIMENTAL REASEARCH DESIGNS:Control Groups, Placebo Control Groups
- GENETICS:Adoption Studies, Twin Studies, Sequential Design, Follow back studies
- RESEARCH ETHICS:Approval for the research project, Risk, Consent
- CAUSES OF ABNORMAL BEHAVIOR:Biological Dimensions
- THE STRUCTURE OF BRAIN:Peripheral Nervous System, Psychoanalytic Model
- CAUSES OF PSYCHOPATHOLOGY:Biomedical Model, Humanistic model
- CAUSES OF ABNORMAL BEHAVIOR ETIOLOGICAL FACTORS OF ABNORMALITY
- CLASSIFICATION AND ASSESSMENT:Reliability, Test retest, Split Half
- DIAGNOSING PSYCHOLOGICAL DISORDERS:The categorical approach, Prototypical approach
- EVALUATING SYSTEMS:Basic Issues in Assessment, Interviews
- ASSESSMENT of PERSONALITY:Advantages of MMPI-2, Intelligence Tests
- ASSESSMENT of PERSONALITY (2):Neuropsychological Tests, Biofeedback
- PSYCHOTHERAPY:Global Therapies, Individual therapy, Brief Historical Perspective
- PSYCHOTHERAPY:Problem based therapies, Gestalt therapy, Behavioral therapies
- PSYCHOTHERAPY:Ego Analysis, Psychodynamic Psychotherapy, Aversion Therapy
- PSYCHOTHERAPY:Humanistic Psychotherapy, Client-Centered Therapy, Gestalt therapy
- ANXIETY DISORDERS:THEORIES ABOUT ANXIETY DISORDERS
- ANXIETY DISORDERS:Social Phobias, Agoraphobia, Treating Phobias
- MOOD DISORDERS:Emotional Symptoms, Cognitive Symptoms, Bipolar Disorders
- MOOD DISORDERS:DIAGNOSIS, Further Descriptions and Subtypes, Social Factors
- SUICIDE:PRECIPITATING FACTORS IN SUICIDE, VIEWS ON SUICIDE
- STRESS:Stress as a Life Event, Coping, Optimism, Health Behavior
- STRESS:Psychophysiological Responses to Stress, Health Behavior
- ACUTE AND POSTTRAUMATIC STRESS DISORDERS
- DISSOCIATIVE AND SOMATOFORM DISORDERS:DISSOCIATIVE DISORDERS
- DISSOCIATIVE and SOMATOFORM DISORDERS:SOMATOFORM DISORDERS
- PERSONALITY DISORDERS:Causes of Personality Disorders, Motive
- PERSONALITY DISORDERS:Paranoid Personality, Schizoid Personality, The Diagnosis
- ALCOHOLISM AND SUBSTANCE RELATED DISORDERS:Poly Drug Use
- ALCOHOLISM AND SUBSTANCE RELATED DISORDERS:Integrated Systems
- SCHIZOPHRENIA:Prodromal Phase, Residual Phase, Negative symptoms
- SCHIZOPHRENIA:Related Psychotic Disorders, Causes of Schizophrenia
- DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:DELIRIUM, Causes of Delirium
- DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:Amnesia
- MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS
- MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS
- PSYCHOLOGICAL PROBLEMS OF CHILDHOOD:Kinds of Internalizing Disorders
- LIFE CYCLE TRANSITIONS AND ADULT DEVELOPMENT:Aging