 |
Abnormal
Psychology PSY404
VU
LESSON
24
ANXIETY
DISORDERS
Anxiety
disorder is the most complex and
mysterious disorder.
Have
you ever experienced
anxiety?
Do
you feel anxious when you
have an exam or a
test?
I
feel anxious going to a hospital for a
check up?
My
friend experiences anxiety visiting
his dentist?
My
student reports anxiety related to attending
his sick mother at an intensive
care unit.
So
what is anxiety?
Anxiety
is a mood- state, characterized by
marked negative affect, bodily
symptoms of tension, restlessness
and
apprehension about
future.
·
Anxiety
is very hard to study. In humans a sense of
uneasiness, looking worried
and anxious.
·
The
physiological response of anxiety is reflected in
increased heart beat and
muscle tension.
·
Anxiety
is not pleasant, it is some
unpleasant thing, usually
students say they can do
well on test if
they
have no examination anxiety.
·
But
moderate amount of anxiety is needed for
optimal performance of people
·
Moderate
anxiety creates a feeling of preparation in
people
·
So anxiety is
future oriented mood
state
·
So when a
student says that I better study hard
for my examination, so as to respond
adequately to
difficult
questions of the exam as well.
·
What
is anxiety?
·
Is it
that anxiety, fear and panic
are the same phenomena? So
let us explore
·
Anxiety
, fear and panic
·
Anxiety
is mood state characterized
negative affect, tension, apprehension of
future.
·
Fear
is an immediate alarm reaction to danger.
It protects us by activating a massive
response
·
In
fear there is an increased
heart beat, blood pressure
and subjective feeling of escape of
an
individual
from danger or terror, so either
flight from or to fight the
enemy.
·
In
fear an individual has
fight- flight response or reaction
situation.
·
Panic
is an abrupt experience of intense
fear or acute discomfort
accompanied by physical
symptoms
of heart palpitations, chest pains,
shortness of breath and
dizziness.
·
Three
basic types of panic
attacks
·
1-Situationally
bound: when you know
you are afraid of high
places or afraid of driving over
long
bridges
you have situation bound
panic disorder (cued).
·
2-
Unexpected: you may experience an
unexpected panic attack disorder
(uncued).
·
3-Situationally
predisposed: you are more
likely to have a panic
attack where you had before.
Both
1
and 2 are included.
·
Panic
and anxiety combine to form different
anxiety disorders
·
1-
Generalized Anxiety Disorder
(GAD)
·
2-
panic with
agoraphobia
·
3-Specific
phobia
·
4-
Social phobia
·
5-Post
Traumatic Stress Disorder (PTSD)
·
6-Obessive
Compulsive Disorder (OCD)
·
Generalized
Anxiety Disorder is unfocused,
prolonged anxiety and
worry.
·
Anxiety
is about minor every day
events
·
Genetics
and psychological factors
responsible for GAD.
·
Panic
with and without
agoraphobia
·
It is
fear and avoidance of
situations considered to be safe
Anxiety is focused on next
panic attack.
·
Agoraphobia
is marketplace or public place
phobia.
·
In
Specific phobia a person
avoids specific situations
that produce severe anxiety or
panic.
108
Abnormal
Psychology PSY404
VU
·
Social
phobias is fear of being around others,
particularly to be in situations that
call for some
kind
of
performance in front of other people
e.g. meeting strangers in
part
·
Post
Traumatic Stress Disorder (PTSD) it
focuses on avoiding thoughts or images of
some past
traumatic
experiences
·
The
PTSD is a traumatic experience and the
intensity of the experience seems to be a
factor in
development.
·
Example
the 8th October 2005,
earthquake affected of our
country show symptoms of
PTSD.
·
Obsessive
Compulsive Disorder (OCD) it focuses on
avoiding frightening or intrusive
thoughts
(obsessive)
·
Leading
to ritualistic behaviors
(compulsions)
·
Washing
and checking of locks,
doors.
·
Influences
in anxiety disorders
·
Biological
influences
·
Behavioral
influences
·
Social
influences
·
Emotional
and cognitive
influences
·
Treatments
for anxiety disorders
·
1-
drug therapy
·
2-Cognitive
behavioral therapy
·
3-Other
treatments
·
Taken
together, the various forms of anxiety
disorders--including phobias,
obsessions,
compulsions,
and extreme worry--represent the
most common type of abnormal
behavior.
·
Anxiety
disorders share several
important similarities with
mood disorders.
·
From
a descriptive point of view,
both categories are defined
in terms of negative
emotional
responses.
·
Stressful
life events seem to play a
role in the onset of both
depression and anxiety.
·
Cognitive
factors are also important
in both types of
problems.
·
From
a biological point of view,
certain brain regions and a
number of neurotransmitters are
involved
in the etiology of anxiety disorders as
well as mood
disorders.
·
People
with anxiety disorders share a
preoccupation with, or persistent
avoidance of, thoughts or
situations
that provoke fear or
anxiety.
·
Anxiety
disorders frequently have a
negative impact on various
aspects of a person's
life.
·
Anxious
mood is often defined in
contrast to the specific emotion of fear,
which is more easily
understood.
·
Fear
is
experienced in the face of real,
immediate danger.
·
In
contrast to fear, anxiety
involves a
more general or diffuses
emotional reaction--beyond
simple
fear--that
is out of proportion to threats
from the environment.
·
Rather
than being directed toward the person's
present circumstances, anxiety is
associated with the
anticipation
of future problems.
·
Anxiety
can be adaptive at low
levels, because it serves as a
signal that the person must
prepare for
an
upcoming event.
·
An
anxious mood is often
associated with pessimistic thoughts
and feelings.
·
The
person's attention turns inward, focusing on
negative emotions and self-evaluation rather
than
on
the organization or rehearsal of adaptive
responses that might be
useful in coping with
negative
events.
Excessive
Worry
·
Worrying
is a cognitive activity that is
associated with anxiety.
109
Abnormal
Psychology PSY404
VU
·
Worry
can be
defined as a relatively uncontrollable
sequence of negative, emotional thoughts
that
are
concerned with possible
future threats or
danger.
·
Worriers
are preoccupied with
"self-talk" rather than unpleasant
visual images.
·
The
distinction between pathological and
normal worry hinges on quantity--how
often the person
worries
and about how many
different topics the person
worries.
·
It
also depends on the quality of
worrisome thought.
·
Excessive
worriers are more likely than
other people to report that the content
of their thoughts is
negative,
that they have less control
over the content and
direction of their thoughts, and
that in
comparison
to other adults, their
worries are less
realistic.
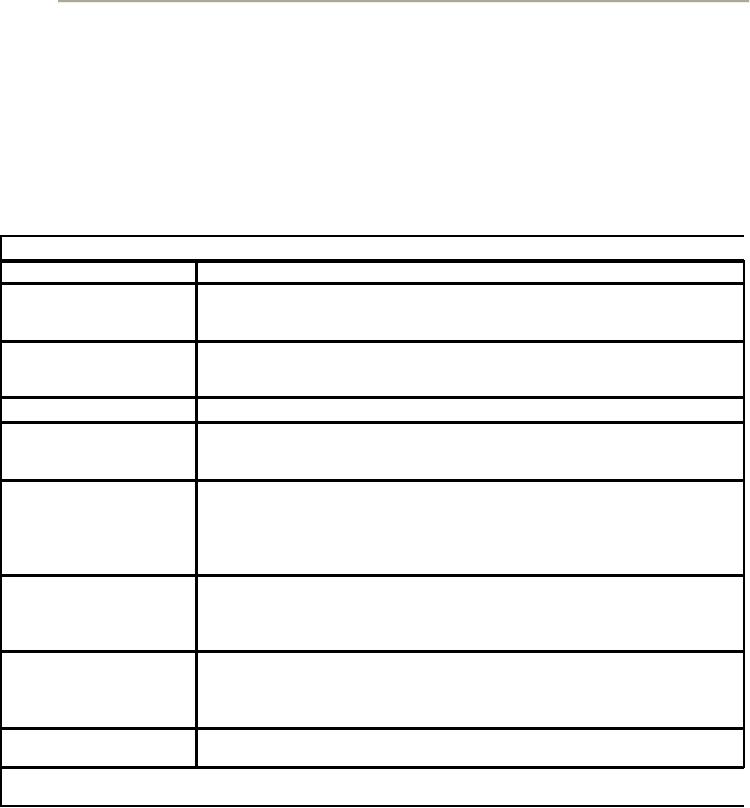
Anxiety
Disorders
Anxiety
Disorder
Description
and Symptoms
Generalized
anxiety disorder Excessive anxiety and
worry that occur on most
days for a period of six
months
(GAD)
about
events ad activities such as work or
school; symptoms include
restlessness,
fatigue,
difficulty concentrating, irritability,
muscle tension, and sleep
disturbance.
Specific
phobia (sometimes Persistent,
excessive, and unrealistic
fear triggered by the presence of a
particular
called
simple phobia)
situation
or object.
Social
phobia
Persistent
and marked fear of one or
more social or performance
situations.
Agoraphobia
The
fear of experiencing the symptoms of
fear and the fear of being in
places from
which
escape might be difficult.
(It is also possible to
experience agoraphobia
without
panic.)
Panic
attack
A
discrete period of intense
fear or discomfort that
appears abruptly and
unexpectedly
and peaks within ten
minutes; symptoms include pounding
heart,
shaking,
trembling, shortness of
breath, sweating, abdominal
distress,
lightheadedness,
and fear of losing control.
Panic attacks can occur
with or without
agoraphobia.
Obsessive-
compulsive
May be defined by either obsessive
or. compulsive symptoms;
obsessions
are
recurrent
disorder
(OCD)
and
persistent thoughts or images that
cause distress and are
experienced as intrusive
and
inappropriate, and compulsions
are
repetitive behaviors that the
person feels driven
to
perform.
Posttraumatic
stress disorder The persistent
experiencing of a traumatic event (e.g.,
in images or dreams) and
the
(PTSD)
avoidance
of stimuli associated with the
trauma; symptoms include
sleep
disturbances,
difficulty concentrating, angry
outbursts, or an exaggerated
startle
response
Acute
stress disorder
Resembles
PTSD, but symptoms persist
for at least two days
but less than
four
weeks
Source:
DSM-IV. Reprinted with permission
from The Diagnostic and
Statistical Manual of Mental
Disorders,
Fourth
Edition. Copyright © 1994 American
Psychiatric Association
·
Is
it normal to be anxious?
·
Almost
everyone can recall at least
one episode of anxious
arousal and fear -- an
experience of
worry
tension, a racing heart, sweaty
palms, or an upset stomach.
Indeed, anxiety and fear can
serve
an
adaptive function: Anxious
arousal tells us to take
special action, to fight what is threatening
us
or
to flee. The fact that most
of us experience some degree of anxiety
suggests that is a part
of
normal
functioning.
·
Is
being entirely anxiety-free
normal or even
desirable?
·
If
we are anxiety free are we
better off?
·
The
answer is no.
110
Abnormal
Psychology PSY404
VU
·
Very
low levels of anxiety, like
high levels, can be detrimental to
performance:
·
With
few exceptions, we perform best
when we experience mild
levels of anxiety.
·
Example
when you have anxiety for
your examination you will be
pushed to study otherwise
you
will
not prepare for
examination.
THE
INTERACTION OF PERSON AND SITUATION
ANXIETY
·
Does
anxiety come entirely from
within the person?
·
Is
it the result of a chemical imbalance or
of maladaptive thinking?
·
Or
is it caused by environmental
conditions?
·
1-Biological
causes
·
The
areas of the brain are
affected by different neurotransmitter
systems, some of which, in
turn,
play
an important role in the experience of
fear and anxiety, and the
way these events
are
interpreted
by the person is important in the shaping
of anxiety disorders. A model of anxiety
disorders
must include biological vulnerabilities
that affect arousal and
activation in interaction
with
personal,
psychological, and environmental
characteristics.
·
·
2-The
diathesis-stress
model, is one
offshoot of this interactional
perspective, which
holds that
individual
dispositions (diathesis) and situational
influences (such as stress) interact to
create and
maintain
psychological disorders (Magnusson &
Ohman, 1987).
THEORIES
ABOUT ANXIETY
DISORDERS
·
Each
of the following theoretical perspectives --
biological, cognitive, behavioral, and
psychodynamic
-- has generated extensive literature on
anxiety and the development of anxiety
disorders.
In addition to the interactional (diathesis-stress)
perspective just described, we
consider
how
these four major perspectives
explain anxiety and anxiety
disorders.
Biological
Theories
·
Anxiety
and the anxiety disorders are
often linked to the body's physical
systems of arousal. In
times
of heightened distress, our bodies
react. When we turn a corner in
our neighborhood and
see
the
smoke of a burning home,
when we receive a phone call
from a hospital late in the evening,
or
when
we see but can't stop a
toddler who is wandering in a busy
parking lot, our bodies do
indeed
react.
·
The
autonomic nervous system carries
messages between the brain
and major organs of the
body
--
the heart, stomach, and
adrenal glands.
In
turn, the adrenal glands
release a hormone, adrenaline
that
activates this system. When
signals of distress are legitimate,
adrenaline galvanizes the
individual
to action. In the absence of crisis, however
excessive adrenaline can
cause anxious
distress.
·
The
biological perspective considers the
roles of genetic and
constitutional factors,
biological
reactivity,
endocrinological and neurotransmitter factors,
and brain anatomy and
functioning in the
development
of anxiety and anxiety disorders.
·
The
term selective association accounts
for the finding that humans
are apparently more
easily
conditioned
to some stimuli than to
others.
·
Based
on this, one hypothesis holds that
humans and many animals
learn fears. Phobias may
be
learned.
·
Medications
for Anxiety Disorders. Because
anxiety symptoms often co-occur
with depression, it should
not
be surprising that some of the
antidepressants also reduce
anxiety.
111
Abnormal
Psychology PSY404
VU
·
Panic
disorders, in particular, respond relatively
well to antidepressants. According to
one published
report,
60 to 90 percent of such patients
display significant improvements when
treated with
antidepressants
(see also Ballenger, Burrows &
Dupont, 1988).
·
In
some cases of posttraumatic
stress disorder, researchers have
claimed that antidepressants
are
effective
as well (Davidson et al.,
1990).
Cognitive
Theories
·
The
basic idea underlying
cognitive approaches is that anxiety
results when we try to
understand
the
events and experiences that
we are a part of in distorted irrational
ways.
·
Ellis
posited that people with unhealthy
emotional lives are also
victims of cognitive irrationality
--
they
view the world based on
self- defeating assumptions.
·
Examples
·
1-To
become afraid on a camping trip
when you are familiar
with the territory of your
camping trip,
is
an irrational fear.
·
2-To
be unwilling to participate in a new game
for fear that you
won't be the absolute best
player is
irrational.
·
**Dog
lovers, when approached by a dog,
might perceive the dog in any of
several ways -- in
terms
of attractiveness, breed, grooming, or
posture. But people with a dog
phobia (an excessive
fear
of dogs) have a narrow and
negative view of dogs,
seeing them in terms of their
size and
ferocity.
They never see the dog's tail
wagging; they see only teeth (Landau,
1980)
·
**Consider
the following example of cognitive
influences in the experience of
deleterious anxiety.
Sam
is waiting for his mother to
pick him up after school.
Most of the other children
have already
gone
home. Sam thinks to himself,
"Why is she late?" In itself, this
thought is not detrimental;
many
children in the same situation
might ask themselves the
same question and he continues
to
worry.
Rather than using the time to
complete a homework assignment or
talk with friends or
teachers,
the anxious youngster engages in
task-irrelevant thought. He may question
why she is late
and
respond by himself due to the fact she
does not love me while the
fact is she is late due
to
traffic
block or car trouble.
·
Anxiety
disorders have multiple
causes and multiple
expressions. As we discussed, several
forces
interact
in the development of disorders of anxiety, and
not all expressions of these
disorders are
the
same. Indeed, several
different types of anxiety disorder
appear in contemporary
classification
schemes.
Behavioral
Theories
Behavioral
explanations of anxiety emphasize the processes
involved in the acquisition of anxiety
responses.
Behaviorists hold that
persons who suffer distressing
levels of anxiety have learned
to
behave
in an anxious manner through
classical conditioning, operant
conditioning, or modeling.
·
Modeling,
also
called observational learning, is another behavioral explanation
for anxiety responses.
Unlike
conditioning, modeling produces learning
without personal experience
with a situation or
object.
Thus, an individual can develop an
emotional response after watching someone
else
experience
an aversive emotional
condition.
Example
**An
adolescent boy observed the
adolescent girl receive the
ridicule from peers might
stay away from
those
same peers hoping to avoid
similar teasing and rejection. He
didn't experience the rejection
directly,
but he observed it and
learned to avoid it from the
vicarious experience.
Behavioral
Therapies
1-
Systematic
Desensitization and exposure
treatments are the treatment of specific
anxiety disorders
these
behavioral techniques typically emphasize
and focus on the client's
cognitive and behavioral
functioning.
112
Abnormal
Psychology PSY404
VU
2-
Rational
Emotive Behavior Therapy the focus is on
modifying the irrational, illogical
belief system.
3-
A
paradoxical intervention encourages the
client to intend or wish for
exactly what is feared.
·
Example I
think I will faint in the examination
hall, you try hard to faint in the
examination hall.
·
The
person does not
faint.
·
The
paradoxical therapists believe
that people's attempts to
solve their problems often
cause them
to
maintain the very problems they are
trying to solve. The
paradoxical therapist thus
provides
directives
that are designed to help
clients give up their "problem-
maintaining solutions".
·
Note
fully discussed in lecture no
26.
113
Table of Contents:
- ABNORMAL PSYCHOLOGY:PSYCHOSIS, Team approach in psychology
- WHAT IS ABNORMAL BEHAVIOR:Dysfunction, Distress, Danger
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Supernatural Model, Biological Model
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Free association, Dream analysis
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Humanistic Model, Classical Conditioning
- RESEARCH METHODS:To Read Research, To Evaluate Research, To increase marketability
- RESEARCH DESIGNS:Types of Variables, Confounding variables or extraneous
- EXPERIMENTAL REASEARCH DESIGNS:Control Groups, Placebo Control Groups
- GENETICS:Adoption Studies, Twin Studies, Sequential Design, Follow back studies
- RESEARCH ETHICS:Approval for the research project, Risk, Consent
- CAUSES OF ABNORMAL BEHAVIOR:Biological Dimensions
- THE STRUCTURE OF BRAIN:Peripheral Nervous System, Psychoanalytic Model
- CAUSES OF PSYCHOPATHOLOGY:Biomedical Model, Humanistic model
- CAUSES OF ABNORMAL BEHAVIOR ETIOLOGICAL FACTORS OF ABNORMALITY
- CLASSIFICATION AND ASSESSMENT:Reliability, Test retest, Split Half
- DIAGNOSING PSYCHOLOGICAL DISORDERS:The categorical approach, Prototypical approach
- EVALUATING SYSTEMS:Basic Issues in Assessment, Interviews
- ASSESSMENT of PERSONALITY:Advantages of MMPI-2, Intelligence Tests
- ASSESSMENT of PERSONALITY (2):Neuropsychological Tests, Biofeedback
- PSYCHOTHERAPY:Global Therapies, Individual therapy, Brief Historical Perspective
- PSYCHOTHERAPY:Problem based therapies, Gestalt therapy, Behavioral therapies
- PSYCHOTHERAPY:Ego Analysis, Psychodynamic Psychotherapy, Aversion Therapy
- PSYCHOTHERAPY:Humanistic Psychotherapy, Client-Centered Therapy, Gestalt therapy
- ANXIETY DISORDERS:THEORIES ABOUT ANXIETY DISORDERS
- ANXIETY DISORDERS:Social Phobias, Agoraphobia, Treating Phobias
- MOOD DISORDERS:Emotional Symptoms, Cognitive Symptoms, Bipolar Disorders
- MOOD DISORDERS:DIAGNOSIS, Further Descriptions and Subtypes, Social Factors
- SUICIDE:PRECIPITATING FACTORS IN SUICIDE, VIEWS ON SUICIDE
- STRESS:Stress as a Life Event, Coping, Optimism, Health Behavior
- STRESS:Psychophysiological Responses to Stress, Health Behavior
- ACUTE AND POSTTRAUMATIC STRESS DISORDERS
- DISSOCIATIVE AND SOMATOFORM DISORDERS:DISSOCIATIVE DISORDERS
- DISSOCIATIVE and SOMATOFORM DISORDERS:SOMATOFORM DISORDERS
- PERSONALITY DISORDERS:Causes of Personality Disorders, Motive
- PERSONALITY DISORDERS:Paranoid Personality, Schizoid Personality, The Diagnosis
- ALCOHOLISM AND SUBSTANCE RELATED DISORDERS:Poly Drug Use
- ALCOHOLISM AND SUBSTANCE RELATED DISORDERS:Integrated Systems
- SCHIZOPHRENIA:Prodromal Phase, Residual Phase, Negative symptoms
- SCHIZOPHRENIA:Related Psychotic Disorders, Causes of Schizophrenia
- DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:DELIRIUM, Causes of Delirium
- DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:Amnesia
- MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS
- MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS
- PSYCHOLOGICAL PROBLEMS OF CHILDHOOD:Kinds of Internalizing Disorders
- LIFE CYCLE TRANSITIONS AND ADULT DEVELOPMENT:Aging