 |
ACUTE AND POSTTRAUMATIC STRESS DISORDERS |
| << STRESS:Psychophysiological Responses to Stress, Health Behavior |
| DISSOCIATIVE AND SOMATOFORM DISORDERS:DISSOCIATIVE DISORDERS >> |
Abnormal
Psychology PSY404
VU
Lesson
31
ACUTE
AND POSTTRAUMATIC STRESS
DISORDERS
What
is stress?
·
Stress
is a process of adjusting to circumstances
that disrupt or threaten a person's
equilibrium.
·
Scientists
define stress
as any
challenging event that requires
physiological, cognitive, or behavioral
adaptation.
·
Stress
is an inevitable, and in some cases a
desirable, fact of everyday
life.
·
Some
stressors, however, are so catastrophic
and horrifying that they can
cause serious
psychological
harm.
·
Such
traumatic
stress is
defined in DSM-IV-TR as an event that
involves actual or threatened
death
or serious injury to self or
others and creates intense
feelings of fear, helplessness, or
horror.
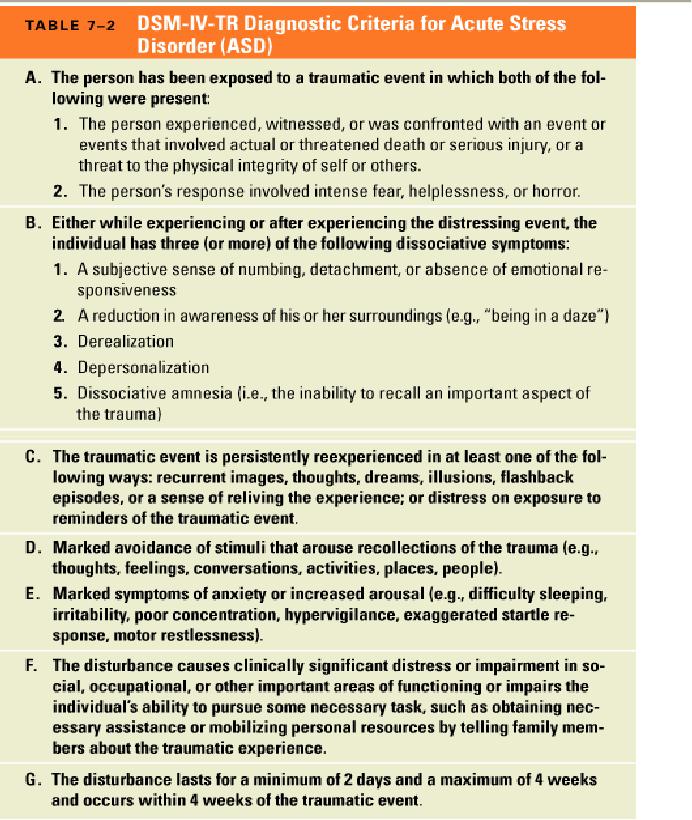
1-Acute
stress disorder (ASD) occurs
within 4 weeks after exposure to
traumatic stress and
is
characterized
by dissociative symptoms, re-experiencing
of the event, avoidance of reminders of
the
trauma,
and marked anxiety or
arousal.
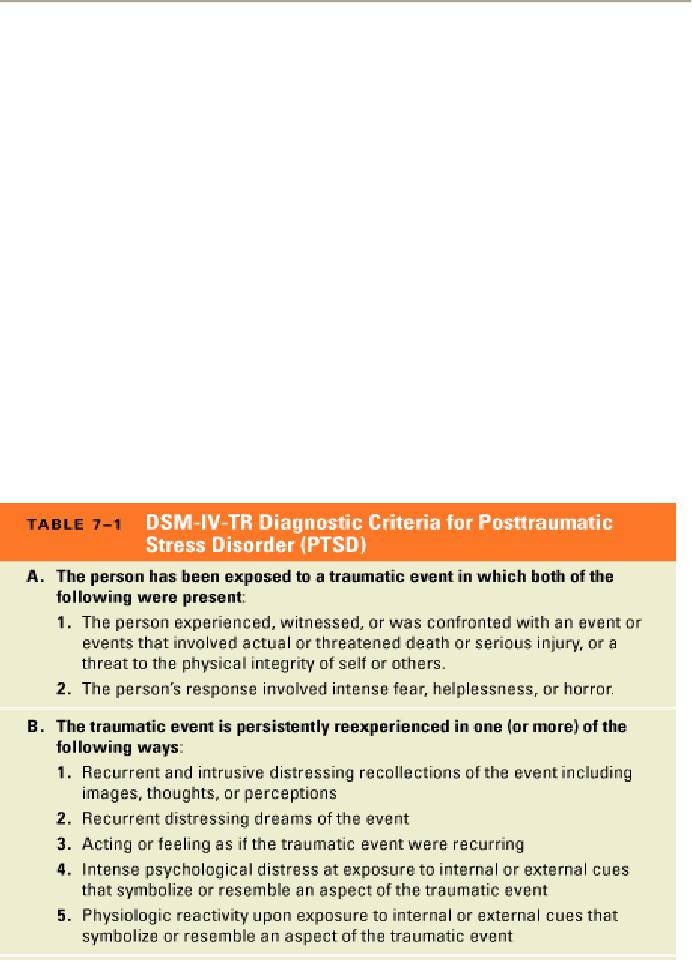
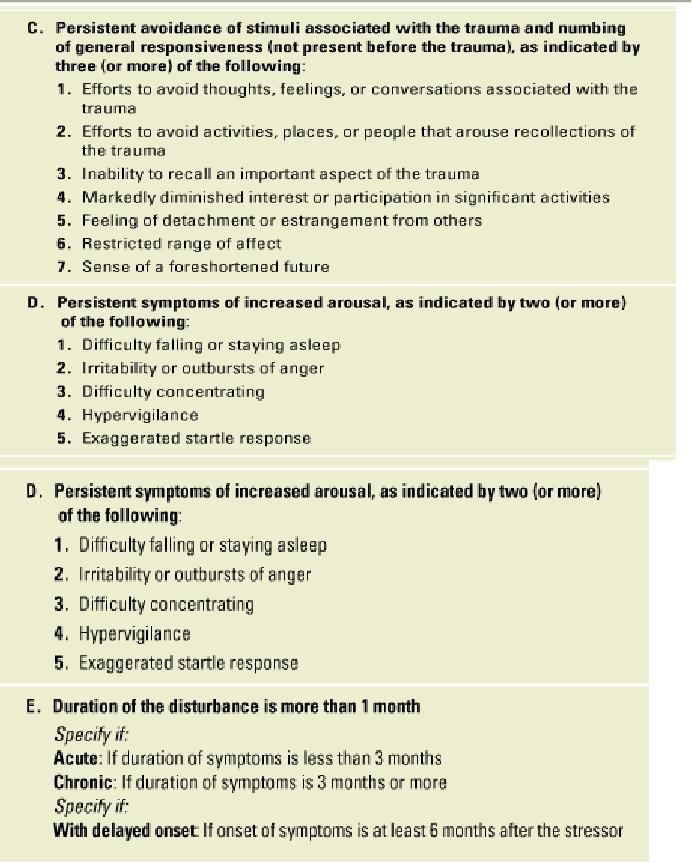
2-Posttraumatic
stress disorder (PTSD) is
also defined by symptoms of
re-experiencing, avoidance,
and
arousal, but in PTSD the symptoms either
are longer lasting or have a
delayed onset.
·
Dissociation
is the disruption of the normally integrated
mental processes involved in
memory,
consciousness,
identity, or perception.
·
The
DSM-IV-TR classifies PTSD as an anxiety disorder,
however, PTSD is of unique importance
and
is characterized by mixed symptoms of anxiety
and dissociation.
Symptoms
of ASD and PTSD
1-People
who have been confronted
with a traumatic stressor
re-experience
the event in a
number of
different
ways.
2-Many
people with ASD or PTSD have
repeated intrusive flashbacks,
sudden
memories during
which
the trauma is replayed in images or
thoughts--often at full emotional
intensity.
3-In
rare cases, re-experiencing
occurs as a dissociative
state, and
the person feels and acts as
if the trauma
actually
were recurring in the moment.
4-Marked
or persistent avoidance of stimuli
associated with the trauma is another
symptom of ASD
and
PTSD. Trauma victims may attempt to avoid thoughts or
feelings related to the event, or they
may
avoid
people, places, or activities that
remind them of the trauma.
5-
PTSD, the avoidance also may
manifest itself as a general
numbing
of responsiveness. People
suffering
from
PTSD often complain that they suffer from
"emotional anesthesia"--their feelings
seem
dampened
or even nonexistent.
6-
Despite their general withdrawal from
feelings, people, and painful
situations, people with ASD
and
PTSD
also experience increased
arousal and anxiety following the
trauma, a symptom which
predicts a
worse
prognosis when it is more
severe.
7-A
number of people with PTSD or ASD also
have an exaggerated
startle response, excessive
fear reactions
to
unexpected stimuli, such as loud
noises.
·
Symptoms
of anxiety and arousal are the
reason why traumatic stress
disorders are grouped
with
the
anxiety disorders in DSM-IV-TR.
·
Acute
stress disorder is characterized by
explicit dissociative
symptoms.
·
Many
people become less aware of
their surroundings following a
traumatic event.
·
They
report feeling dazed, and they
may seem "spaced out" to
other people.
8-Other
people experience depersonalization,
feeling cut
off from themselves or their
environment.
People
with this symptom may report
feeling like a robot or as if they were
sleepwalking.
9-Derealization
is
characterized by a marked sense of
unreality about yourself or the world
around you.
·
ASD
also may be characterized by
features of dissociative
amnesia, specifically
the inability to recall
important
aspects of the traumatic
experience.
147
Abnormal
Psychology PSY404
VU
·
DSM-IV-TR
lists a sense of numbing or
detachment from others as
dissociative symptoms
that
characterize
acute stress disorder.
·
A
very similar symptom is listed as an
indicator of avoidance, not
dissociation, in the diagnosis of
PTSD.
·
This
discrepancy in diagnostic criteria
reflects some of the broader controversy
about whether ASD
and
PTSD should be classified as dissociative or anxiety
disorders.
Diagnosis
of ASD and PTSD
·
Maladaptive
reactions to traumatic stress
have long been of interest
to the military.
·
Historically,
most of the military's concern has
focused on battle dropout, that
is, men who
leave
the
field of action as a result of what has
been called "shell shock" or
"combat neurosis."
·
During
the Vietnam War, however, battle dropout
was less frequent than in
earlier wars, but
delayed
reactions to combat were
much more common.
·
This
change prompted much
interest in PTSD, a condition
first listed in the DSM in 1980
(DSM-
III).
·
The
basic diagnostic criteria for
PTSD--re-experiencing, avoidance, and
arousal--have remained
more
or less the same in revisions of the
DSM.
·
However,
two significant changes in the
classification of traumatic stress
disorders were made
with
the
publication of DSM-IV in 1994:
Acute stress disorder was included as a
separate diagnostic
category,
and the definition of trauma
was altered.
·
The
diagnostic criteria for ASD
and PTSD are essentially the
same.
·
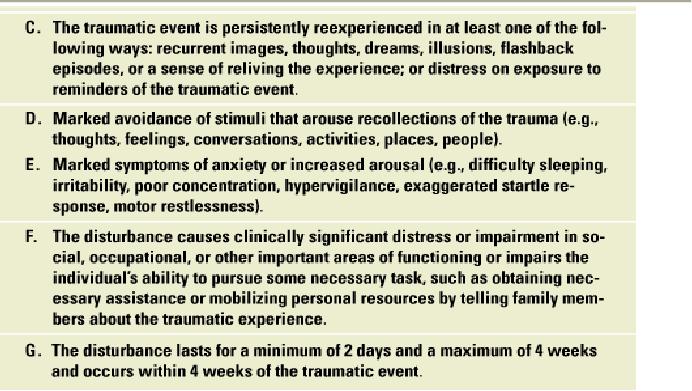
The
two exceptions are that
ASD explicitly includes
dissociative symptoms and
lasts no longer than
4
weeks, whereas PTSD continues
for at least 1 month after a
trauma or it has a delayed
onset.
·
Not
surprisingly, many people suffer from ASD
after experiencing trauma, and the
presence of
ASD
may predict future PTSD.
148
Abnormal
Psychology PSY404
VU
149
Abnormal
Psychology PSY404
VU
150
Abnormal
Psychology PSY404
VU
·
Earlier
versions of DSM defined
trauma as an event "outside the range of
usual human
experience.
·
Even
before September 11, however, researchers
discovered that, unfortunately, many
traumatic
stressors
are a common
part
of human experience in the United
States today.
·
Thus
DSM-IV-TR defines trauma as
(1) the experience of an event involving
actual or threatened
death
or serious injury to self or
others and (2) a response of
intense fear, helplessness, or horror
in
reaction
to the event.
·
The
psychological effects of exposure to
natural or man-made disasters, like
September 11 or the
Oklahoma
City bombing in 1995 are of
great concern.
·
September
11 also called attention to the
trauma experienced by emergency
workers.
Frequency
of Trauma, PTSD, and
ASD
1-The
National Comorbidity Survey
found that nearly 8 percent
of people living in the United
States
will
experience PTSD at some point in
their lives, including about 10
percent of women and 5
percent
of
men.
2-Research
finds that women are
especially likely to develop PTSD as a
result of rape, while
combat
exposure
is a major risk factor for PTSD among
men.
·
PSTD is
also commonly found among
crime victims.
·
Still,
the single most common cause
of PTSD is the sudden, unexpected death
of a loved one.
·
In
general, trauma does not
occur completely at random.
·
The
development of PTSD following a trauma is
also not random.
·
Researchers
have found that people who
suffer from ASD are more
likely to develop PTSD
subsequently.
·
The
prediction is far from
perfect, however, and two
caveats bear special
scrutiny.
·
First, people
with subclinical
ASD,
that is, with symptoms
that are not severe or
pervasive enough to
meet
diagnostic criteria, nevertheless are at
greater risk for PTSD than
trauma victims with
relatively
few psychological
symptoms.
·
Second,
the different symptoms of ASD
are not equally good in
predicting future PTSD.
·
The
presence of three symptoms--numbing,
depersonalization, and a sense of
reliving the
experience--are
the best predictors of PTSD.
·
Other
research shows how the
symptoms of PTSD diminish gradually as
time passes.
151
Abnormal
Psychology PSY404
VU
·
However,
PTSD can be a chronic disorder.
·
Scientists
studying social factors and the risk
for PTSD have focused
primarily on (1) the nature
of
the
trauma and the individual's level of
exposure to it and (2) the
availability of social
support
following
the trauma.
·
Victims
of trauma are more likely to
develop PTSD when the trauma is more
intense, life-
threatening,
and involves greater
exposure.
·
As
with less severe stressors,
social support after a trauma can play a
crucial role in alleviating
long-
term
psychological damage.
·
A
lack of social support is
thought to have contributed to the
high prevalence of PTSD
found
among
Vietnam veterans.
·
In
an analysis of more than
4,000 twin pairs,
researchers found that MZ twins
had a higher
concordance
rate than DZ twins for experiencing
trauma, specifically exposure to
combat.
·
Following
exposure to trauma, identical twins also
had higher concordance rates
for PTSD
symptoms
than did fraternal twins.
·
A
very different line of research
focuses on the biological consequences
of
exposure to trauma
and
how
these consequences may play a
role in the maintenance of PTSD.
·
People
with PTSD show alterations in the
functioning and perhaps even
the structure of the
amygdala
and hippocampus, two
biological findings consistent,
respectively, with the experience
of
heightened
fear reactivity and intrusive
memories.
·
Other
evidence finds that PTSD is
associated with increased
levels of circulating
norepinephrine
and
general psychophysiological arousal,
for example, an increased
resting heart rate.
·
Together,
the pattern of biological findings
suggests that the sympathetic
nervous system is
aroused
and
the fear response is sensitized in
PTSD.
·
The
heightened reactivity may be due to the
failure of the stress response
system to shut down.
·
According
to two-factor theory, classical
conditioning creates
fears
when the terror inherent
in
trauma
is paired with the cues associated
with the traumatic
event.
·
Operant
conditioning, in turn, maintains
the
fears.
·
Specifically,
when fear-producing situations are avoided, the
avoidance is negatively reinforced by
the
reduction of anxiety.
·
More
recent psychological perspectives
focus on individual differences in the
risk for ASD and
PTSD.
·
In
addition to preexisting mental health
problems, research indicates
that cognitive factors such
as
expectancies,
preparedness, and control influence the
risk for PTSD following a
trauma.
·
Some
theories suggest that
dissociation is an unconscious defense
that helps victims to cope
with
trauma.
·
However,
research indicates that
dissociation is associated with
more not less PTSD.
·
Dissociation
may not be adaptive, but
most theorists agree that
victims of trauma must, over
time,
find
a balance between gradually
facing their painful emotions
while not being overwhelmed by
them.
·
Psychologist
Edna Foa, a leading PTSD researcher,
has highlighted the importance of
emotional
processing,
which
involves facing fear, diminishing
its intensity, and coming to
some new
understanding
about the trauma and its
consequences.
·
Integrating
the experience of trauma with broader
memories and beliefs
involves the task of meaning
making--finding
some broader reason or higher value
for enduring the trauma.
·
The
combined evidence suggests alternative
pathways can lead to ASD
and PTSD.
·
Anyone
might develop ASD or PTSD given a critical level of
exposure and a trauma of
sufficient
intensity.
·
The
development of PTSD results from a
combination of factors, including
personality
characteristics
that predate the trauma,
exposure during the trauma,
and emotional processing
and
social
support afterwards.
152
Abnormal
Psychology PSY404
VU
Prevention
and Treatment of ASD and
PTSD
·
The
potential for preventing PTSD is so
important that the federal
Emergency Management
Agency,
the government agency that deals
with natural and manmade
disasters, is required to
provide
special funding to community mental
health centers during
disasters.
·
Perhaps
the most widely used early
intervention is critical incident stress
debriefing (CISD), a
single
1
to 5 hour group meeting
offered within 1 to 3 days
following a disaster.
·
CISD
involves several phases
where participants share their
experiences, reactions, group
leaders
offer
education, assessment, and referral if
necessary.
·
Since
World War I, interventions
with soldiers who drop
out of combat have been
based on the
three
principles of offering (1) immediate
treatment in the (2) proximity of the
battlefield with the
(3)
expectation of return to the front lines
upon recovery.
·
The
trauma of combat and the
structure of the military make
generalization of these principles
to
other
traumas difficult, but the
goals are logical ones to
modify to fit the unique circumstances
of
other
traumas.
·
Few
studies of the treatment of ASD have
been conducted, a circumstance
that is not
surprising
given
that the diagnosis was developed
only recently.
·
Nevertheless,
some research indicates that
structured interventions with
ASD can
lead
to the
prevention
of future PTSD.
·
Psychotherapists
who specialize in PTSD suggest
some general principles for the
psychological
treatment
of the disorder.
·
In the
order in which they are
likely to be addressed in therapy, these
include
1)
Establishing a trusting therapeutic relationship
2)
Providing education about the process of coping
with trauma
3)
Stress-management training
4)
Encouraging the re-experience of the trauma
and
5)
Integrating the traumatic event into the
individual's experience.
153
Table of Contents:
- ABNORMAL PSYCHOLOGY:PSYCHOSIS, Team approach in psychology
- WHAT IS ABNORMAL BEHAVIOR:Dysfunction, Distress, Danger
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Supernatural Model, Biological Model
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Free association, Dream analysis
- PSYCHOPATHOLOGY IN HISTORICAL CONTEXT:Humanistic Model, Classical Conditioning
- RESEARCH METHODS:To Read Research, To Evaluate Research, To increase marketability
- RESEARCH DESIGNS:Types of Variables, Confounding variables or extraneous
- EXPERIMENTAL REASEARCH DESIGNS:Control Groups, Placebo Control Groups
- GENETICS:Adoption Studies, Twin Studies, Sequential Design, Follow back studies
- RESEARCH ETHICS:Approval for the research project, Risk, Consent
- CAUSES OF ABNORMAL BEHAVIOR:Biological Dimensions
- THE STRUCTURE OF BRAIN:Peripheral Nervous System, Psychoanalytic Model
- CAUSES OF PSYCHOPATHOLOGY:Biomedical Model, Humanistic model
- CAUSES OF ABNORMAL BEHAVIOR ETIOLOGICAL FACTORS OF ABNORMALITY
- CLASSIFICATION AND ASSESSMENT:Reliability, Test retest, Split Half
- DIAGNOSING PSYCHOLOGICAL DISORDERS:The categorical approach, Prototypical approach
- EVALUATING SYSTEMS:Basic Issues in Assessment, Interviews
- ASSESSMENT of PERSONALITY:Advantages of MMPI-2, Intelligence Tests
- ASSESSMENT of PERSONALITY (2):Neuropsychological Tests, Biofeedback
- PSYCHOTHERAPY:Global Therapies, Individual therapy, Brief Historical Perspective
- PSYCHOTHERAPY:Problem based therapies, Gestalt therapy, Behavioral therapies
- PSYCHOTHERAPY:Ego Analysis, Psychodynamic Psychotherapy, Aversion Therapy
- PSYCHOTHERAPY:Humanistic Psychotherapy, Client-Centered Therapy, Gestalt therapy
- ANXIETY DISORDERS:THEORIES ABOUT ANXIETY DISORDERS
- ANXIETY DISORDERS:Social Phobias, Agoraphobia, Treating Phobias
- MOOD DISORDERS:Emotional Symptoms, Cognitive Symptoms, Bipolar Disorders
- MOOD DISORDERS:DIAGNOSIS, Further Descriptions and Subtypes, Social Factors
- SUICIDE:PRECIPITATING FACTORS IN SUICIDE, VIEWS ON SUICIDE
- STRESS:Stress as a Life Event, Coping, Optimism, Health Behavior
- STRESS:Psychophysiological Responses to Stress, Health Behavior
- ACUTE AND POSTTRAUMATIC STRESS DISORDERS
- DISSOCIATIVE AND SOMATOFORM DISORDERS:DISSOCIATIVE DISORDERS
- DISSOCIATIVE and SOMATOFORM DISORDERS:SOMATOFORM DISORDERS
- PERSONALITY DISORDERS:Causes of Personality Disorders, Motive
- PERSONALITY DISORDERS:Paranoid Personality, Schizoid Personality, The Diagnosis
- ALCOHOLISM AND SUBSTANCE RELATED DISORDERS:Poly Drug Use
- ALCOHOLISM AND SUBSTANCE RELATED DISORDERS:Integrated Systems
- SCHIZOPHRENIA:Prodromal Phase, Residual Phase, Negative symptoms
- SCHIZOPHRENIA:Related Psychotic Disorders, Causes of Schizophrenia
- DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:DELIRIUM, Causes of Delirium
- DEMENTIA DELIRIUM AND AMNESTIC DISORDERS:Amnesia
- MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS
- MENTAL RETARDATION AND DEVELOPMENTAL DISORDERS
- PSYCHOLOGICAL PROBLEMS OF CHILDHOOD:Kinds of Internalizing Disorders
- LIFE CYCLE TRANSITIONS AND ADULT DEVELOPMENT:Aging